Pilonidal sinus is a condition that affects the area just above the buttocks called the natal cleft. When loose hairs fall off from the neck and back, they accumulate in the natal cleft. Sometimes, they make small holes in the skin or get into the existing pores. Hairs carry bacteria and thus they can infect the holes or pores of the skin. At times, the infection results in the formation of an abscess or a discharge that is released out onto the skin through a tunnel called the sinus.
Treatment
Occasional discharge can be treated with antibiotics but surgery is the most effective way to remove pilonidal sinus. The operation is performed under general anesthesia and lasts for about half an hour. The surgeon removes the sinus along with the infected tissue.
Complications
Sometimes, surgery for the pilonidal sinus can cause general complications like pain, bleeding, scarring and the formation of blood clots. Other complications may be a partial breakdown of the wound, numbness around the wound and slow healing.
Recovery
Pilonidal Sinus Treatment in HSR Layout is performed as an outpatient procedure and the patient is discharged the same day. Convalescence takes about two to three weeks, after which one can resume normal activities. Exercising in this period may speed up recovery. Talk to your doctor about an optimal workout regimen. Occasionally, pilonidal sinus makes a comeback.
Laparoscopic Surgeon in HSR Layout | Dr. Manas Tripathy says Gastric Banding is a treatment for obesity, a growing in India. A person is officially obese when he or she attains a Body Mass Index (BMI) of more than 30 kg/m2. Lifestyle alterations remain the main forms of treating obesity, but in an ‘instant results’ world, more and people are opting for surgery to battle their body mass. Gastric banding or lap-band surgery is one such surgical technique to treat obesity.
Lap-Banding is short for Laparoscopic Adjustable Gastric Banding (LAGB). This surgery uses a laparoscope to place an adjustable silicone doughnut-shaped belt or band around the upper part of the stomach. The band can be tightened from the outside by filling it with saline. The silicone band is connected to a port, which is placed just under the skin of the abdomen. The saline is passed into or removed from the band through this port.
LAGB works on the psychiatric side. The idea is to restrict the size of the stomach and limit the amount of food it can hold, while simultaneously slowing the passage of food to the intestines. This results in the gut sending signals to the brain of satiety even with the consumption of less food. The signal is actually sent from a small pouch created by the band on the upper stomach. When the pouch is filled with saline, the same signal is sent to the brain with still less food in the stomach.
Who needs a Lap-Band?
The Lap-Band is an actual brand name, which has now become generic like Kleenex. Lap-bands come in different sizes and models manufactured by various companies. People with a BMI of 40 kg/m2 or who are 45 kgs. above their ideal body weight qualify for LAGB. LAGB can also be performed on people with a BMI of 35-40 kg/m2 if the patient suffers from weight-related medical conditions like high blood pressure, diabetes or hypertension.
Most Laparoscopic Surgeons like Dr. Manas Tripathy will only recommend gastric banding if the patient has a history of failed attempts at weight loss with lifestyle changes. The procedure is off-limits for children or teenagers below 18. Everyone undergoing the procedure must display a full understanding of the technique and must be willing to adopt the lifestyle changes that are associated with the procedure. This is where our center helps with counseling and assessment of psychology to assure the patient meets these criteria.
LAGB is not recommended for people who have difficulty understanding the technique, are emotionally unstable or are addicted to drugs or alcohol. Patients with a history of gastrointestinal problems like ulcers need to be evaluated carefully before LAGB can be prescribed for them. Some underlying medical conditions like those of the heart and lungs can put patients at a high-risk for surgery and will not undergo the procedure.
People with a BMI of over 50 kg/m2, will be asked to reduce before undergoing LAGB. The risks of the procedure in such patients may outweigh the benefits of the surgery. There is a growing discussion about providing LAGB to diabetics with a BMI of 35-40 kg/m2, but there is no consensus or any surgical guidelines for this group, which makes them ineligible.
LAGB Surgery Procedure
The surgery is performed under general anesthesia and lasts between 1 and 2 hours. Again, the surgeon makes several small incisions in the abdomen. The surgeon inserts a port into one of the incisions through which a tiny telescopic camera is inserted into the abdominal cavity. The camera transmits the internal images on a television screen. Surgical instruments are inserted through the other incisions. These instruments place the band in its identified location and perform other aspects of the operation guided by the Laparoscopic Surgeon in HSR Layout | Dr. Manas Tripathy. The gastric band and the port are set into their place with sutures.
Preparing for LAGB
Proceedings before the surgery vary from center to center. Many medical centers insist on a commitment from patients to make the mandatory alterations to their lifestyle and eating habits before scheduling the procedure. Patients may be recommended to alter their eating habits before the surgery itself by eating 5 to 6 small meals a day to prepare them mentally for the challenges post-LAGB. Doctors may also wean the patient off high-calorie snack desserts like ice cream and milkshakes. These desserts may be highly restricted after surgery since they can be easily absorbed despite the stomach tightness after surgery.
If there are other medical complications, doctors may put patients under preoperative risk-reduction programs. Furthermore, a weight reduction of 5% to 10% before the surgery has been shown to produce better post-operative results.
Recovery after Lap-Band Surgery
LAGB generally requires shorter hospitalization and faster recovery than gastric bypass operations, recovery varies between patients. Most people are able to resume work a week after the procedure and it might take up to six weeks before they can return to pre-operative levels of activity.
Gastric Band Adjustments
The gastric band adjustment is commonly called the lap-band ‘fill’. After LAGB, there is a convalescence period of 6 to 8 weeks, after which the first ‘fill’ of the lap band. It involves infusing a saline solution into the lap band through the port that was left under the skin, which is connected to the band. There may be a change in appetite before the first fill. Fills are painless and usually conducted by the same surgeon who performed your operation. These adjustments are made to augment weight loss, particularly if it has reached a plateau. Loosening the band may a good way to adjust to managing nausea and vomiting.
Life after Lap-Band Surgery
Weight reduction after LAGB is a gradual process; initially, the loss of weight may be faster-1 or 2 kilos per week. However, this would eventually level up to a more modest weight loss of half a kilo per week. Now is the time to stick to your pre-surgery commitment because the foods you eat will directly decide how much and how fast you will lose weight. The weight loss tends to become significantly slower after about 18 months. Average weight reduction in the first year is 40% of the excess body weight with a 10% to 20% weight loss in the following year. Patients are advised to keep in regular touch with their surgeons during this time because further band adjustments may be required
Side Effects and Complications
Common side effects of lap-band surgery include nausea, vomiting, development of ulcers at the site of the band, indigestion, constipation, dehydration and also regaining of weight. Since LAGB is a stomach-restricting technique, which does not interfere with the absorption of nutrients, there are no vitamin deficiencies generally. Still, many centers recommend multivitamin supplements.
LAGB has a relatively low risk of complications as compared to other surgical weight reduction surgeries. There is a possibility of the band malfunctioning, slipping or dissolving into the stomach. Other complications may include but are not limited to, infection, bleeding and abdominal pain.
The Surgeon
It is important that the surgeon who is to perform lap-band surgery on you is a qualified bariatric surgeon, preferably with a good track record. You can also ask how frequently he or she conducts LAGB procedures; a count of about 100 or more procedures annually indicates popularity and he or she is more likely to give you a good result. A surgeon who is part of a multi-specialist team of nurses, nutritionists, pre-and post-operative counseling who also meets the criteria above should be your preferred surgeon.
Welcome to the Podcast Series “Proctology and Laparoscopic Surgery”. This is Dr. Manas Tripathy, the Laparoscopic Surgeon in Koramangala, Bangalore with you.
In today’s podcast episode, I would like to discuss “How to prevent Gallstones?”
A tumor in a stomach may need part of the stomach to be removed. In order for a surgeon to do that, he or she needs to know the precise location of the tumor inside the stomach. The surgeon also needs to see the tumor in order to decide how much (or maybe all) of the stomach has to be resected or removed. The doctors will discuss with you beforehand.
Symptoms of Stomach Tumour
Nausea, vomiting Abdominal pain Weight loss, weakness The above symptoms do not necessarily indicate the presence of a tumor. However further tests may establish that. Non-surgical treatment like radiotherapy or chemotherapy is generally ineffective in managing stomach cancer and surgery is usually required. If the tumor spreads beyond the stomach, the oncologist will discuss other treatment options for you.
Before Laparoscopic Gastrectomy
Patients will be subject to several tests and examinations before the procedure. These can include standard blood tests, urine analysis, endoscopy (the doctor looks down your throat by inserting a small telescope attached to a camera, barium swallow x-ray, a nuclear medicine scan and a CT Scan of the abdomen. Some regular medications may have to be stopped one week prior to the operation. Smokers and drinkers will also have to cease their vices.
Laparoscopic Gastrectomy
The procedure is similar to all other laparoscopic procedures. The surgeon makes 4-5 small incisions on the abdomen and inserts a narrow tube (port) in one of the incisions. The surgeon releases a gas (mostly carbon dioxide) into the abdomen through another incision. As a result, the abdomen is inflated so the surgeon can better see the interior on camera. The laparoscope is a tiny telescope attached to a camera, which is inserted into the abdomen through the port. The camera transmits the internal images on a television screen.
Surgical instruments are inserted through the rest of the incisions, which are used to remove the part of the stomach where the tumor is located. The surgeon then expands one of the incisions and removes the part, which is kept in a plastic bag. If the entire stomach has been removed or it is no longer functional, the surgeon attaches the small intestine directly to the esophagus with surgical staplers, so that the patient can eat again. The carbon dioxide and other instruments are now removed through the incisions, which are closed with stitches, steri-strips or glue-like bandages.
Complications of Gastrectomy
Gastrectomy has the potential to manifest the following complications and perhaps others not mentioned below:
Infection of the skin at one of the small ports sites Leakage of the connection between the stomach and small bowel Collection of pus inside your abdomen (intra-abdominal abscess) Postoperative ileus (the intestines slow down/stop working for several days) Small bowel obstruction (kinking of the small bowel, causing blockage) Pneumonia
Convalescence and Recovery
Patients are usually discharged 3 to 4 days after the laparoscopic gastrectomy. Your bowels should be fully functional by the time you can go home. You should limit strenuous activity or heavy lifting for about a month.
Call Your Surgeon
Consult your surgeon immediately if you experience any of the following:
High fever Severe abdominal pain Odor or increased drainage from your incision No bowel movements for three days
Diagnostic Laparoscopy is generally performed under general anesthesia but can also be performed under local anesthesia in certain cases. The surgeon and anesthetist will discuss with you the type of anesthesia will be safer and more comfortable for you. Local anesthesia is usually injected into the affected organ. For, e.g., if it is an abdominal condition, local anesthesia will be given into the skin of the abdominal wall. The drug will numb the entire region to enable painless incision and safe insertion of the laparoscope. Patients just feel a ‘bee sting’ before small doses of sedatives are administered intravenously. This puts the patient into what is referred to as ‘twilight sleep’, a state in which they are asleep but not in deep slumber.
Once the patient falls into the required depth of sleep, gas is released into the abdominal cavity to enlarge it in order for the surgeon to get a better view of the internal proceedings. The common gases are a nitrous oxide or laughing gas or carbon dioxide. There is little risk of ill-effects of the gas, which is removed from the abdomen after the operation.
Diagnostic laparoscopy is performed under general anesthesia if the patient is ineligible for surgery under ‘twilight sleep’ or for those who opt for it. General anesthesia is usually preferable for patients who are young, those who are unable to lie still or are afflicted with a medical condition, which makes general anesthesia a safer option
Pre-Laparoscopy Preparations
Most of the diagnostic laparoscopy is performed as outpatient procedures, meaning you can go home on the day of the procedure itself. You will not be allowed to eat or drink for a period of time before the laparoscopy, the duration of which will be decided by the surgeon and anesthesiologist.
Patients are required to arrive 1-2 hours before the scheduled laparoscopy. They will undergo certain tests like a blood test, urine analysis or x-ray before the procedure. You can shower on the morning of the procedure or on the night before.
Patients who take regular medication should discuss them with the doctor at the time of scheduling the procedure. The surgeon may disallow you take some of them immediately prior to the procedure. If you are on non-critical drugs like aspirin, blood thinners, arthritis medicine, the doctor will tell you when to stop taking them before the laparoscopy.
If you have been operated upon under sedatives, you will someone to drive you home after the procedure. Sedatives affect your reflexes and judgment for as much as 12-20 hours. You will not be allowed to drive any vehicle, even a two-wheeler until the following day.
The Procedure
The patient is either given local anesthesia and sedation or general anesthesia, after which the patient goes to sleep. The surgeon makes small incisions on the organ and inserts a narrow, tube-like instrument called a port inside the cavity. The laparoscope is a tiny telescope, which is connected to a camera, is then inserted through the port. The camera then provides a magnified view of the patient’s interior body parts on a television screen.
Other ports are inserted through the other incisions made, which give your surgeon the details and exact nature of your condition. This allows him or her to make a proper diagnosis and formulate the best treatment plan. After this, the surgeon removes all the instruments from the body and closes the incisions with sutures, which will be absorbed by the body or with surgical tapes.
After the Laparoscopy
Patients are transferred to a recovery room after the procedure where they are continuously monitored. The sedatives and anesthesia will take some time to wear off, even after patients are fully awake. You will be discharged once the effects of the drug have worn off enough to let you get out of bed and walk without assistance. As mentioned above, you must have someone to drive you home.
Expect some soreness around the incisions for some time. The pain will gradually subside, even as you take pain relievers. Most of the patients will be able to shower the next day after the laparoscopy, though you may need to cover the incision site with a plastic cover to prevent it from coming into contact with water. Patients generally return to their normal activities within a week. The surgeon will inform you in case there are certain restrictions in your case.
A follow-up examination is mandatory two weeks after the laparoscopy.
Possible Complications
Medical and surgical procedures can be prone to complications, the most common being infection and bleeding. After a laparoscopy, other complications that can arise, but are not limited to, include injury to the site and neighboring organs. Patients suffering from ascites may experience temporary leakage.
Consult your Doctor Immediately If:
Your condition reaches any of the following:
1.Fever above 101 degrees F (39 C) 2.Drainage from or redness any of your incisions 3.Continued nausea or vomiting 4.Increasing abdominal swelling 5.Bleeding 6.Chills 7.Persistent cough or shortness of breath 8.Inability to urinate 9.Pain not controlled by medication
Laparoscopic anti-reflux procedures are surgeries for heartburns. Moderate to severe heartburn may prompt your doctor to advise a laparoscopic anti0reflux surgery to treat your gastroesophageal reflux disease or GERD, the technical name for heartburn.
What is GERD?
The term ‘heartburn’ is generally used to describe a variety of digestive issues. However, all of them are symptoms of Gastroesophageal Reflux Disease. In GERD, stomach acids back up or reflux into the esophagus causing heartburn. The primary symptom is a burning sensation between the ribs or just below the neck. The sensation may radiate into the throat and neck through the chest. Other symptoms can include vomiting, difficulty in swallowing and persistent coughing and wheezing.
The Cause of GERD
The lower esophageal sphincter muscle is naturally weak in some people. Others make it weak by excessive intake of spicy and fatty foods, certain medications, smoking, alcohol consumption, tight clothes, and vigorous exercising. Sometimes, changed body positions like lying down or bending over may also cause the LES to relax and cause the reflux. Many patients suffering from GERD develop what is termed a hiatal hernia. This hernia develops when the top part of the stomach juts upwards into the chest cavity through the diaphragm. This condition is thought to contribute to the acid reflux. If GERD requires surgery, it also repairs the hiatal hernia.
Contributors to GERD
The lower esophageal sphincter muscle is naturally weak in some people. Others make it weak by excessive intake of spicy and fatty foods, certain medications, smoking, alcohol consumption, tight clothes, and vigorous exercising. Sometimes, changed body positions like lying down or bending over may also cause the LES to relax and cause the reflux. Many patients suffering from GERD develop what is termed a hiatal hernia. This hernia develops when the top part of the stomach juts upwards into the chest cavity through the diaphragm. This condition is thought to contribute to the acid reflux. If GERD requires surgery, it also repairs the hiatal hernia
Lifestyle Changes: Changes in dietary habits can reduce the frequency and severity of heartburn. Changes in lifestyle may also include losing weight, quitting smoking, reduce alcohol consumption and alteration in eating and sleeping patterns.
Medication
If heartburn persists despite the lifestyle changes, drug therapy will be required. Antacids can neutralize stomach acids, while other medications, available over the counter, reduce the production of stomach acids. A doctor can also prescribe certain medicines to alleviate symptoms by healing the esophagus.
Surgery
Patients who fail to respond to lifestyle changes and medication or those who do not wish to be continuous medication may consider surgery, which is effective in permanently treating GERD. The most common surgical procedure is a fundoplication or Nissen fundoplication, after the surgeon who introduced the procedure in the late 1950s. In a fundoplication, first the hiatal hernia is repaired, if present. Then, the top part of the stomach is wrapped around the base of the esophagus to strengthen the lower esophageal sphincter (LES). This reinforces the one-way valve function of the LES to prevent the acid reflux.
The operation can be an open surgery with a single, long incision on the upper abdomen. The alternative is a laparascopic surgery with several small incisions and inserting surgical instruments in the abdomen for the actual surgery telecast on a TV screen.
In a laparoscopic procedure, the actual operation is conducted within the body’s organs. In laparoscopic anti-reflux surgery, the surgeon makes small incisions on the abdomen, in which he inserts narrow, tube-like instruments called trocars. Sometimes, the abdomen may be enlarged with carbon dioxide for better maneuverability within the abdomen. The laparoscope, connected to a tiny camera, is also inserted in the abdomen. The surgeon conducts the operation by looking at the proceedings on a television screen.
Open Anti-Reflux Surgery
Certain cases may not be suitable for the laparoscopic method due to various reasons like the inability to handle to organs safely. Factors, which may indicate open surgery, may include obesity, previous abdominal surgery with present scar tissue or excessive bleeding. The choice between laparoscopic and open surgery is made by the surgeon. There are times when the surgeon begins a laparoscopic procedure and midway switches to open surgery if he feels that it is safer.
Laparoscopic Anti-Reflux Surger
Advantages of Laparoscopic Anti-Reflux Surgery
reduced postoperative pain shorter hospital stay a faster return to work improved cosmetic result Is the Laparoscopic Method Suitable for You?
As we have seen above, despite its benefits, the laparoscopic procedure is not safe or practical for everyone. Your general physician or a gastroenterologist, in consultation with a surgeon trained in the laparoscopic method whether this procedure is suitable for you. You may have to undergo a complete physical evaluation to enable the specialists to make an informed decision.
Preparing for Laparoscopic Anti-Reflux Surgery
If the laparoscopic method has been found suitable for a patient, the surgeon will discuss the potential risks and benefits of the operation and obtain his or her signed consent. There will be several medical examinations prior to surgery like blood tests, chest x-rays and EKG depending on the patient’s age and medical condition.
The patient will be advised to take a shower on the night before or on the morning of the operation. The patient will not be allowed any food or drink after midnight of the night before the operation except medications with a sip of water in the morning before surgery. Drugs such as anti-inflammatory medications, blood thinners, aspirin, Vitamin E, etc. will not be allowed for up to a week prior to surgery.
The Day of the Surgery
Patients usually arrive at the hospital on the day of the surgery, though some may arrive on the eve of surgery. Pre-operative medicine will be administered via a small needle or catheter by a qualified support staff member. The operation will be performed under general anesthesia and can last for several hours. Following the operation, patients are usually taken to their wards and monitored until they wake up.
After Open or Laparoscopic Anti-Reflux Surgery
At home during convalescence, patients should not undertake any strenuous activity and avoid lifting heavy weights. Post-operative pain is normally mild but some patients might require pain medications, which will be prescribed by the surgeon.
In most cases, patients need to alter their diet. Surgeons usually prescribe a liquid immediately after the operation and gradually progressing to solid foods. Patients usually resume their normal activities within a short span of time. A follow-up examination will be necessary two weeks after the operation.
Side Effects of the Surgery and Complications
There are generally no long-term side effects of GERD surgery. Some people experience difficulty in swallowing immediately after surgery, but it usually subsides within one to three months. Patients may also be restricted in belching or vomiting, while some patients have reported bloating of the stomach. These complain are usually temporary and are naturally resolved within months.
As with most other surgical procedures, there can be a complication with GERD surgery as well. Some patients may experience the following complications, while there can be other, less common complications as well:
Your surgeon will discuss all of this with you prior to surgery. These factors also help patients decide whether the risks outweigh open or laparoscopic surgery vis-à-vis non-surgical treatment.
Adverse reaction to general anesthesia Bleeding Injury to the esophagus, spleen, liver, stomach or other internal organs Infection of the wound, abdomen, or blood Sometimes, patients may need a procedure for stretching the esophagus called endoscopic dilation. In rare cases, the patient may need a second procedure or report no improvement in their GERD symptoms. Even after a complete cure, reflex symptoms may reappear in the long run.
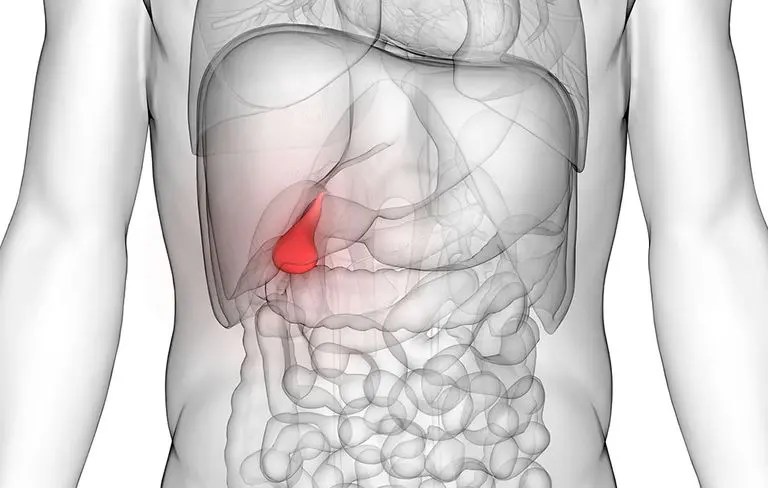
Gallstones are small stones that develop in the gall bladder. The condition is quite common and is also genetic in many cases. The chances of developing gall bladders increase with age. People who eat a fat-rich diet are particularly susceptible to it. The ailment can cause severe symptoms; the most common is returning attacks of shooting abdominal pain
Treatment
Gallstones can be dissolved or disintegrated into tiny pieces but these treatments involve the use of drugs with possible side effects. Besides, there is a high rate of failure. In many cases, the gallstones form again. Antibiotics can heal infections of the gall bladder due to the stones. A low-fat diet can also help in preventing pain. However, alleviation of symptoms is temporary.
Surgery
Laparoscopic surgery for gallstones or cholecystectomy is a procedure, in which the gall bladder (and gallstones) is removed. After making incisions in the abdomen, the surgeon will inflate the abdomen with carbon dioxide, in order to see the interior more clearly. The surgeon then inserts a telescope, which is attached to a video camera. This will guide him (through a video monitor) while inserting more surgical instruments in the other incisions in order to remove the gall bladder. Before removing the bladder, the surgeon may take a special x-ray (intraoperative cholangiography) to see the locations of the bile ducts inside the liver.
After surgery, the bile will flow from the liver into the small intestine through the common bile duct. Since the gallbladder has been removed, the body will no longer be able to store bile between meals. This has little or absolutely no effect on the process of digestion in the majority of people.
There may be some complications as with most surgeries. In a few laparoscopic cholecystectomies, the surgeon may switch to open surgery, if a larger incision is required. These can cause additional complications like scars, inflammation, and bleeding. More serious complications may include:
Development of a hernia at the surgery site Injuries to nearby abdominal structures Surgical emphysema Leaking of bile or leftover stones Chronic pain Diarrhea Bowel injury Damage to the liver
Recovery
Patients are generally discharged the following day. Convalescence may take between two to four weeks depending on the extent of surgery and your type of occupation. Check with the surgeon before the operation about how much you can exercise. For the first few days, increasing how much you walk is recommended. You can expect a full recovery and be able to eat normally during recovery.
An epigastric hernia develops when fat juts out through a weakness in the abdominal wall between the umbilicus and sternum. The result is lump or hernia, which can be painful, particularly if the fat is pinched by the wall of the abdomen.
Treatment
The most common and popular treatment for a hernia is surgery. An operation is the quickest way to repair a hernia, particularly if the bulge is growing bigger. Timely surgery also preempts any serious complications that can accompany inguinal hernia. Sometimes, the hernia can be controlled with a padded belt called a truss. However, a hernia will not go away without surgery.
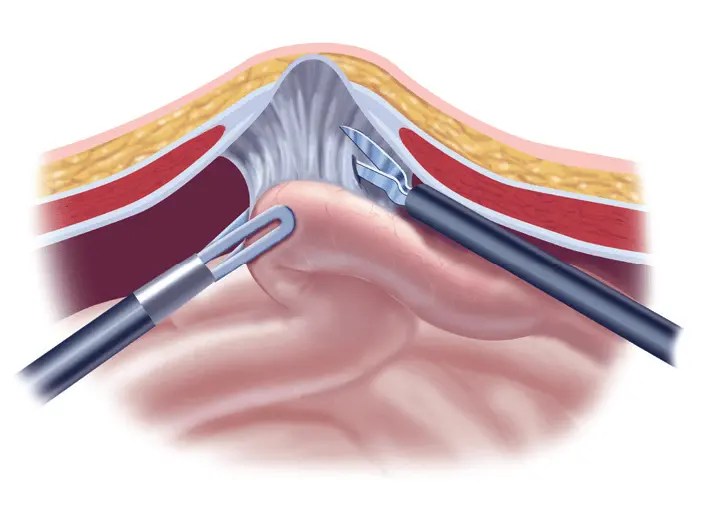
Epigastric Hernia surgery can involve any anesthetic techniques depending on the situation. The surgeon makes an incision in the abdomen and simply removes the ‘hernia sac’. The muscle layer is strengthened with sutures. A synthetic mesh will also be used to fortify the weak spot. The operation usually lasts for about three-quarters of an hour.
Surgical Procedure
The operation to repair an epigastric hernia involves general anesthesia and is usually over in about half an hour. The surgeon makes a cut on the hernia and frees the ‘hernial sac’. The surgeon will either remove the fat tissue or push it back. If tissues from the abdomen are also pushing through, they are placed back within the abdomen. The weak spot through which the fat pushed through to create the hernia is closed with stitches. For larger hernias, the weak spot is reinforced with a synthetic mesh.
Complications
General side effects that may afflict the patient are the same as those after other hernia fixing surgeries. More serious complications may include:
Development of a lump at the surgery site
Injuries to nearby abdominal structures
Patients are generally discharged the same day. Convalescence may take between two to four weeks depending on the extent of surgery, after which you can resume normal activities. Check with the surgeon before the operation about how much you can exercise. For the first few days, increasing your walking is recommended. Occasionally the hernia can recur
Welcome to the Podcast Series “Proctology and Laparoscopic Surgery”. This is Dr. Manas Tripathy, Laparoscopic Surgeon in HSR Layout, Bangalore with you.
In today’s podcast episode, I would like to discuss “Gallstones”
Gallstones are small stones that develop in the gall bladder. The condition is quite common and is also genetic in many cases. The chances of developing gallbladders increase with age. People who eat a fat-rich diet are particularly susceptible to it. The ailment can cause severe symptoms; the most common is returning attacks of shooting abdominal pain
So, today’s podcast is very important. Listen to it carefully to know more about “Gallstones”.
Welcome to the Podcast Series “Proctology and Laparoscopic Surgery”. This is Dr. Manas Tripathy, the Laparoscopic Surgeon in Bangalore with you.
In today’s podcast episode, I would like to discuss “Non-Surgical Treatment for Gallstones”
Gallstones are one of the most common gastrointestinal conditions caused by too must production of cholesterol and bilirubin. People try using home remedies provided by their loved ones.
Don’t self-medicate. Self-medication may lead to more serious problems.
Consult your Laparoscopic Surgeon for Gallstones treatment.
So, today’s podcast is very important. Listen to it carefully to know more about “Gallstones”.